Delayed Zinc Toxicosis in a Starved Dog
The below case illustrates a rapid onset of critical illness in a severely malnourished stray dog. After initial support turned this too-weak-to-walk stray into a bouncing puppy and he regained his appetite, he rapidly deteriorated in our ICU due to zinc toxicity from pennies that presumptively had been in his empty stomach for some time.
Presentation:
A young, intact male pitbull was brought to our hospital by Animal Control Officers in late September. No microchip was found and postings were made on social media sites searching for the owner to no avail. In the meantime, we named him Mac.

Physical examination:
On physical examination, he was 7.0kg (about 7kg underweight), had a temperature of too low to read, HR 110bpm, RR 20 with clear lungs, CRT 3 seconds, and pink/tacky gums. He was mentally dull, emaciated with a BCS of 1/9, too weak to walk, and was suffering from fecal and urinary scald, ulceration of the paws and mouth, pressure sores, and fly strike.
Initial labwork and support:
Point of care labwork on presentation showed a blood glucose of 40mg/dL and PCV/TS 52%/4.4. His renal values were normal and he was mildly acidotic (pH 7.3) and had a lactate of 2.2mmol/L. He was supplemented with dextrose and intravenous fluids and rapidly rebounded. He started eating within a few hours. Additionally, he was started on Clavamox, Capstar, Panacur, and his wounds treated.
Day One:
Feedings were started slowly at 1/3rd of his resting energy requirements (RER) based on current weight: 7 kg x 30 + 70 = 280 calories/day divided by 3 = 93.3 calories on Day 1. (Another equation for RER = 70(7kg)3/4 = 301 calories/day). Based on the calories in Hill’s I/D (376 calories/ 13 oz can), this puppy was fed 1 tablespoon every 6 hours. He had a wonderful appetite and energy level rapidly improved after a few meals.
Day Two:
Suddenly, the puppy started urinating red and became lethargic. A urine sample was obtained via free catch and centrifuged to differentiate hematuria from pigmenturia. The supernatant of the spun urine remained red. Could this be myoglobinuria from this severe catabolic state (breaking down muscle due to starvation) or muscle injury from fleeing danger or more likely hemoglobin due to hemolysis? At this point, full labwork was obtained to determine the cause of this pigmenturia.
This chart can help differentiate hematuria, myoglobinuria, and hemoglobinuria based on urine evaluation:
| Hematuria | Pigmenturia | |||||
| Color | Red | Red | ||||
| Post-spun supernatant color | Clear | Red | ||||
| Cause | RBCs | Hemoglobin or Myoglobin
Note: evaluate blood plasma color to differentiate:
(generally what occurs in most cases) |
Labwork:
NOVA blood gas was performed along with a recheck PCV/TS. Salient changes included a drop in PCV to 40% from 52%. This could be attributed to rehydration but the TS actually rose from 4.4 to 5.0g/L. Additionally, lactate rose to 4.2 from 2.2 mmol/L. Upon examination of the hematocrit tubes, the plasma was found to be pink. Supportive care continued for the next several hours with planned recheck of bloodwork and imaging, if needed.
At the next check in 4 hours, a full complete blood count and chemistry panel were performed. The urine remained red and the Mac took a severe turn for the worst. He stopped eating, became remarkably nauseated, and became more subdued and weak. CBC revealed normal WBC and platelet counts, however, the HCT dropped to 30%. Chemistry panel revealed BUN 30mg/dL (9-29), Cholesterol of <50mg/dL, ALT 648 U/L (0-120), GGT 30 U/L (0-14), ALP 165 U/L (0-140), Tbili 4.1 (0-0.3). CPK, phosphorus, glucose, and potassium are normal. Spun PCV/TS = 22%/5.4. Microscopic evaluation of the blood smear did not reveal hemoparasites and saline auto-agglutination was negative. Plasma was now red and the urine remained red as well.
Differential diagnoses:
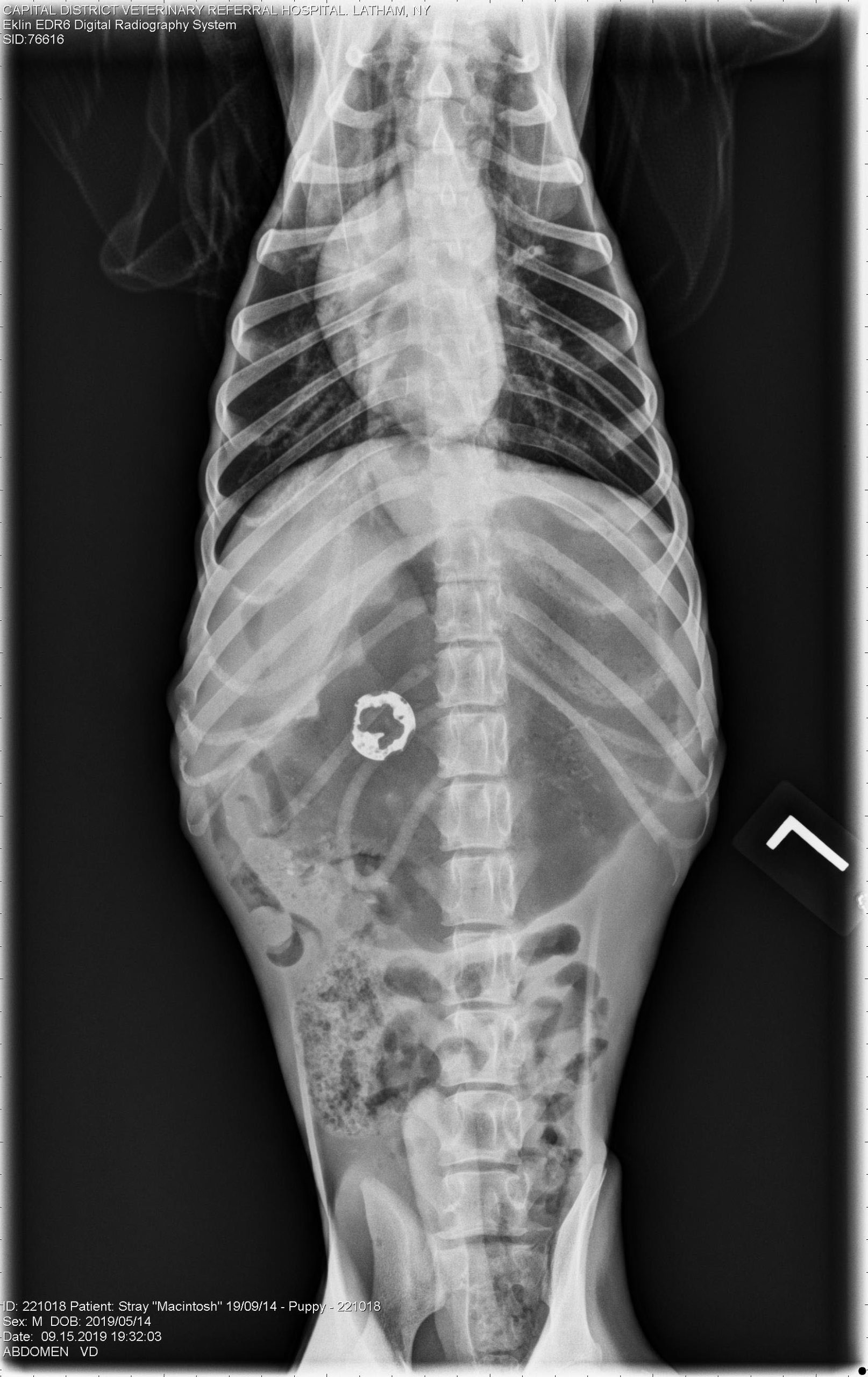
With this stray dog, a wonderful rescue stepped forward to take financial responsibility for Mac. Therefore, we laid out the possible differential diagnosis since some clearly have a better prognosis than others to set forth a plan. Our facts are: an emaciated and re-fed dog, falling PCV, hemoglobinuria, elevated ALT, GGT, ALP, hyperbilirubinemia, and hypocholesterolemia. The most common rule outs for the anemia, hyperbilirubinemia, and hemoglobinuria include immune-mediated hemolytic anemia, zinc toxicosis, onions, garlic, snake envenomation, and Leptospirosis (due to hemolysins with phospholipase activity). On top of that, we have elevated liver values and low cholesterol which can be seen together in liver failure (which Lepto can also cause). However, the hypocholesterolemia in this dog is likely secondary to chronic malabsorption and Leptospirosis is always seen with azotemia so this was unlikely. Elevated liver values due to acute liver injury can be seen with both IMHA and zinc toxicity. We did the next most logical step and took abdominal radiographs to search for a penny.
Abdominal radiographs:
 Radiologist conclusions:
Radiologist conclusions:

- Gastric distention with foreign material (including metallic foreign body). A gastric outflow tract obstruction is not seen at this time.
- Fluid and gas distended call thoracic esophagus on the venture dorsal image. Differential diagnostic considerations would include a sliding hiatal hernia or gastroesophageal reflux.
- Decreased serosal margin detail consistent with the young age and the nature of the dog.
Plan:
After administering ~10ml/kg packed RBC transfusion, Mac underwent endoscopy for attempted removal of the penny and other gastric foreign materials (shoe strings, plastic, cloth), but this procedure necessitated conversion to exploratory and gastrotomy due to the adherence of the disintegrated penny to the mucosa. He recovered well and found himself a loving home!


Zinc Toxicosis
Each penny minted after 1982 contains elemental zinc (~2440mg) covered by a copper coating. As discussed, zinc toxicosis can cause hemolytic anemia which can lead to hemoglobinemia and hemoglobinuria. Other zinc sources include nuts, bolts, and zinc oxide-based skin creams, such as diaper rash cream and sunscreen. There is a recent case report of zinc toxicity from the ingestion of a Holiday Garland. The exact mechanism of the hemolysis is unknown, although it is suspected to be secondary to direct damage to red blood cell membranes and inhibition of RBC biochemical mechanisms.
Absorption of zinc from the penny is enhanced by an acidic gastric environment. Mac’s penny was undergoing a very slow absorption without causing toxicity as seen from his normal hematocrit on presentation. With the introduction of food his gastric pH dropped causing rapid zinc absorption and the rest is history. This is the author’s first experience with an insidious zinc toxicosis as most dogs present to the emergency for clinical signs such as weakness due to severe anemia (as they are typically not starved).
Treatment options:
Endoscopic or surgical removal is essential. At times, induction of emesis for penny retrieval can be successful, typically for a recent and witnessed ingestion. We did attempt this with Mac without success. Failure of the zinc concentration to decline after penny removal suggests that there is still zinc in the gastrointestinal tract or that renal insufficiency is preventing zinc excretion. Although a recent case report demonstrated safety and success, chelation for residual zinc removal is considered controversial because chelating agents may increase gastrointestinal absorption of zinc and can be nephrotoxic. Instead, intensive supportive care is recommended sometimes requiring dialysis. It is important to note that charcoal is ineffective.
Conclusion:
Our conscientious doctors were most worried about such issues as overfeeding or refeeding syndrome in this starved dog, however, as usual, the unexpected occurred. It is very interesting that the penny remained undigested (or very slowly digested) in Mac’s stomach for an unknown amount of time but within 24 hours of introduction of food massive absorption occurred. Presumably, his gastric acid very poorly and slowly was eroding the copper coating. Additionally, it is known that low dietary essential fatty acid levels, intestinal parasitism, malabsorptive syndromes, and chronic enteritis may decrease intestinal zinc absorption and we know Mac was experiencing at least one of these things (malabsorption).
In the average dog, the penny’s copper protective coating is eroded quickly by acid. With feeding, gastric acid is secreted due to the presence of food in the stomach. This will decrease the pH of the gastric lumen disintegrate the copper coating to free the zinc. Food itself likely doesn’t play a big role. In fact, some foods such as rice, cereals, and corn actually reduce zinc absorption. In hindsight and x-ray vision, day 1 aggressive gastric acid reduction with a famotidine CRI or proton pump inhibition may have reduced the rapidly of Mac’s decompensation, although the penny would still have needed removal.
It is helpful to keep an open mind and flexibility with our differential diagnoses and treatment plans in these very unpredictable veterinary patients!
References:
Bischoff K, Chiapella A, Weisman J, Crofton L, Hillebrandt J. Zinc Toxicosis in a Boxer Dog Secondary to Ingestion of Holiday Garland. J Med Toxicol. September 2017;13(3):263-266.
Cummings JE and Kovacic JP. The ubiquitous role of zinc in health and disease. JVECC. June 2009; 19(3).
Gurnee CM and Drobatz KJ. Zinc intoxication in dogs: 19 cases (1991-2003).
J Am Vet Med Assoc. April 2007;230(8):1174-9.
Lee Y, Kane M, Park, H. Treatment of zinc toxicosis in a dog with chelation using D-penicillamine. JVECC. 20 Nov 2015; 26(6).
Lonnerdal B. Dietary Factors Influencing Zinc Absorption. The Journal of Nutrition. May 2000; 130 (5): 1378S–1383S.